




Heart failure
1. Anatomy of heart
The heart is a muscle consists of 4 cavities:
2 atrias
2 ventricles
On a functional level, the heart is divided into 2 contiguous parts within the same organ:
the right heart
the left heart
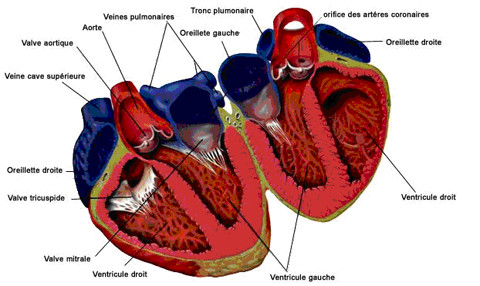 |
The left heart sends the oxygenated blood to the various tissues of the body through the aorta artery (main artery distribution) and the smaller arteries. Once used by the tissues, the oxygen-depleted blood back to the right heart, first by small veins, then the veins caves (major veins) that serve as the collector. It is then sent to the lungs. Once oxygenated in the lungs, blood returns to the left heart for distribution throughout the body. Thus, the loop is closed.
According to the concerned part of the heart, there are 2 types of bloodstream:
- small circulation (pulmonary)
- big circulation (systemic)
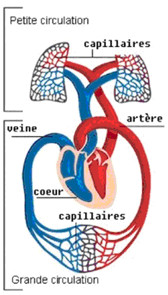 The small circulation.
The small circulation.
This is the pulmonary circulation. It includes the right heart (atrium and right ventricle), pulmonary artery, lungs and pulmonary veins. It allows blood to refill oxygen.
The systemic circulation.
It includes the left heart (atrium and left ventricle) and aorta (the large artery leaving the left ventricle) which will distribute oxygen throughout the body especially the vital organs: brain, kidney, liver etc...
3. Definition of heart failure
Heart failure is a condition in which the heart is no longer able to perform its pumping work properly to cover the energy needs by the body. Cardiac output (the quantity of blood ejected per minute by the heart) no longer allows the body to function normally.
What is following :
- a decrease in blood vasculature downstream
- congestion of the bloodstream in the venous back system
This failure may be the reflect of:
- or a systolic dysfunction: abnormal contraction of the heart muscle
- or a diastolic dysfunction: abnormal ventricular filling
If the deficiency relates to both the previous two mechanisms, there is talk of a systolic and diastolic dysfunction.
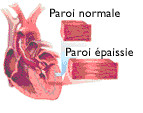 At the beginning, heart failure does only little symptoms or sometimes there is no symptoms. The heart find in itself the resources to cope with the increased workload imposed on it. It adapts by becoming thicker (hypertrophy) is the compensated stage.
At the beginning, heart failure does only little symptoms or sometimes there is no symptoms. The heart find in itself the resources to cope with the increased workload imposed on it. It adapts by becoming thicker (hypertrophy) is the compensated stage.
 But little by little, this adaptation becomes inadequate and reaches its limits. The heart expands, becomes less and less capable to ensure the needs of the organism and the clinical manifestations appear. Worse yet, the compensation mechanisms put in place by the body will be deleterious for the heart.
But little by little, this adaptation becomes inadequate and reaches its limits. The heart expands, becomes less and less capable to ensure the needs of the organism and the clinical manifestations appear. Worse yet, the compensation mechanisms put in place by the body will be deleterious for the heart.
According to the affected part of the heart, there are 2 types of heart failure:
- left heart failure or left ventricular failure when failure reached the left ventricle.
- right heart failure or right ventricular failure when the failure reaches the right ventricle.
When failure is simultaneously right and left hearts, we speak of a congestive heart failure
The rapid heartbeat (tachycardia) is a common clinical sign of heart failure. Depending on the type of deficiency, the symptoms can be different:
Left Heart Failure
The blood no longer escape to the stagnant bodies in the vessels of the lungs. Clinical signs are mainly respiratory.
- The first stage consists of dyspnea (shortness of breath) when performing efforts.
- Dyspnea occurs then with varying degrees of effort less and less important to appear even at rest.
- At the final stage, the patient is always short of breath, a cough with bloody sputum, can no longer sleep lying down and breathing better when sitting.
Although these symptoms usually develop gradually, the trend may be more brutal in some cases: these are the episodes of hemodynamic pulmonary edema in which the patient literally drowns in the liquid transudation resulting from congestion of blood in blood vessels of the lungs. It is said that currently the patient has "water in the lungs".
The right heart failure
The return of venous blood to the heart and / or the ejection of blood to the lungs is no longer effective. Blood stagnates in the body, resulting in:
- edema
- Hepatomegaly: liver enlargemen
- ascites: ccumulation of fluid in the abdomen
The main symptoms are fatigue and taking undue weight.
The diagnosis of heart failure is based on :
- History (patient interview)
- Analysis of the patient's medical history
- Physical examination (review os system)
- Electrocardiography gives an idea of the impact of heart failure on the performance of the heart and can helps to determine the cause (sequelae of myocardial infarction)
- Echocardiography to evaluate cardiac functional capacity of the ventricles (cardiac function).
- The chest radiography (cardiomegaly)
- The continuous recording (Holter) can search for cardiac arrhythmias.
Other tests may be performed in hospitals: examinations hemodynamic (cardiac catheterization), biological, histological, bacteriological, parasitic, immunological, etc.
The causes are multiple. All conditions that weaken the heart muscle, which interfere with blood circulation, or that require the heart to work faster or stronger (anemia, hyperthyroidism, arterio-venous shunt) can lead to heart failure.
The main causes of heart failure are:
- Myocardial infarction: part of the heart muscle is destroyed. The heart has less force to shrink.
- High blood pressure: the increase in blood pressure causes thickening of the muscular walls of the left ventricle. This thickening restricts the free movements of heart and makes it more rigid. It can not contract or relax effectively.
- Cardiac arrhythmias: the heart muscle contractions are more effective because they are either too fast or too slow or out of sync.
- Insufficiency of the aortic valve: the aortic valve is no longer able to close and blood reflux into the left ventricle during diastole. Accordingly, the amount of blood sent to the organs and tissues is less.
- Narrowing (stenosis) of the aortic valve or the pulmonary valve: it causes an obstruction to the passage of blood through the valves at the corresponding contraction of the ventricles.
- Insufficiency of the mitral valve or tricuspid valve: blood flowed toward the atria when the ventricles contract. As a result, the amount of blood sent to the organs or the lungs is less.
- Narrowing (stenosis) of the mitral valve and tricuspid valve: it causes an obstruction to the passage of blood through the valves at the corresponding filling of the ventricles during diastole. The blood stagnates and leads upstream congestion atria.
- Infections of the heart muscle or heart valves: myocarditis, endocarditis.
- Disorders of the pericardium (envelope of the heart): fluid Pericarditis, Constrictive Pericarditis
- Toxic cardiomyopathy: alcoholic cardiomyopathy, cardiomyopathy post-chemotherapy.
- Infiltrative cardiomyopathy: Cardiac amyloidosis, hemochromatosis
- Heart defects: inter-ventricular and inter-atria communication, obstructive cardiomyopathy.
- Lung: pulmonary embolism, chronic pulmonary insufficiency, pulmonary infections, pulmonary fibrosis.
7. Classification of heart failure
It is based on an assessment prepared by the functional NYHA (New York Heart Association) in the USA .
The criteria for the classification is used to evaluate the importance of the functional impact of the disease, to determine the type of treatment to administer to patients with heart failure.
There are 4 classes of heart failure :
| Classes | Fonctional evaluation |
|---|---|
| Classe I | No limitation of physical activity. Habitual physical activity does not create excessive fatigue, dyspnea or anginal pain. |
| Classe II | Moderate limitation of physical activity. No symptoms at rest, but usual physical activity causes fatigue, dyspnea or anginal pain. |
| Classe III | Marked limitation of physical activity. No symptoms at rest but physical activity lower than normal (light effort) causes fatigue, dyspnea or anginal pain. |
| Classe IV | Unable to perform any physical activity without discomfort. Symptoms of heart failure or angina occur sometimes even at rest. The discomfort is increased by any physical activity. |
The evolution and prognosis depend on the disease responsible for the heart failure.
The most common consequences of the heart failure are:
- Cardiac arrhythmias: atrial fibrillation, ventricular arrhythmias
- Thromboembolic events
- Renal failure
- Digestive disorders: anorexia, nausea
- Neurological disorders: insomnia, agitation
- Cardiogenic shock as manifested by circulatory collapse
- Death
9. Traitement
Dietary guidelines: They are used to remove all factors that can adversely affect heart failure: tobacco aggravates pulmonary signs, excessive alcohol consumption, obesity which is in itself an overload for the heart.
Restriction of salt: This is an important element as the ingested salt contributes to the retention of fluid. It is recommended the cardiac patient to weigh every day because any abnormal weight gain will require an adjustment of medical treatment by the treating physician.
Rest: It is indicated in acute heart failure. In some cases (acute myocardial infarction), the strict bed rest may be indicated for optimal treatment.
Medications
- Diuretics help to eliminate excess of salt and have a vascular effect. Spironolactone showed a benefit on mortality in patients severely affected by severe heart failure
- Inhibitors of angiotensin converting enzyme 2 (ACE) . They have a dual action, vascular and neuro-hormonal. They dilate both the arteries and veins without altering cardiac output. They correct a number of hormonal abnormalities that contribute to the occurrence and persistence of heart failure. Antagonist of receiver of angiotensin 2 (AT2) are part of the treatment of heart failure and can be administered to patients with side effects caused by the ACE inhibitors.
- Beta-blockers: they slow the heart and correct some disorders of the nervous system (the sympathetic nervous system) that maintain and exacerbate heart failure.
- Digoxin can be administered to improve the patient's symptoms.
- Amiodarone (Cordarone) may be administered in case of disturbance of heart rhythm (atrial fibrillation).
- Anticoagulant treatment can be administered in cases of cardiac arrhythmias (atrial fibrillation, atrial flutter) or preventive (low molecular weight heparin) to prevent venous thrombosis especially in bedridden patients
Pleural puncture or puncture of ascites (evacuation of serous effusions in hospital) can improve symptoms of patients.
The automatic implantable defibrillator, electro-systolic heart training , heart transplant and artificial heart is the ultimate treatment methods.
The main drugs to avoid
- Anti-inflammatory drugs (NSAID)
- Anti-arrhythmic class I
- Calcium channel blockers
- Tricyclic antidepressants
Physical activity: Patients with stable heart failure should have a physical activity and training adapted to the effort (cardiac rehabilitation) to improve their tolerance to effort and quality of life.
Pregnancy: Pregnancy is unlikely to be completed in patients with heart failure class III or IV, because of the high risk of morbidity and mortality.
Heart failure is a serious disease, often with debilitating and life-threatening risk. Patients who are not treated effectively face a higher risk of death. To increase their chances of survival, people with heart failure should keep strictly to the dietary guidelines and therapeutic established by their physician.
11. References
1. SWEDBERG K.
Guidelines for the diagnosis and treatment of chronic heart failure: executive summary (update 2005) The Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology
European Heart Journal 2005 26(11):1115-1140
2. Société Européenne de Cardiologie
Recommandations pour le diagnostic et le traitement de l'insuffisance cardiaque chronique
Arch Mal Cœur Vaiss 2002 ; 95 : 5-53.
3. HUNT SA, BAKER DW, CHIN MH, et al.
ACC/AHA guidelines for the evaluation and management of chronic heart failure in the adult: executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to revise the 1995 Guidelines for the Evaluation and Management of Heart Failure)
J Am Coll Cardiol 2001; 38:2101-13